

Documentation is more than a formality in chiropractic care – it’s the foundation for clinical accuracy, compliance, and patient trust. Proper charting not only protects your practice but also supports better outcomes and streamlined billing.

The Importance of Accurate Chiropractic Documentation
Every adjustment, exam, and patient encounter tells a story. Accurate documentation provides that narrative – it explains what was done, why it was done, and how the patient responded.
Why It Matters
- Legal Protection: Proper documentation ensures your care decisions are defensible.
- Insurance Reimbursement: Clear, compliant notes speed up claim approvals.
Patient Continuity: Consistent record-keeping helps other providers follow your care plan.
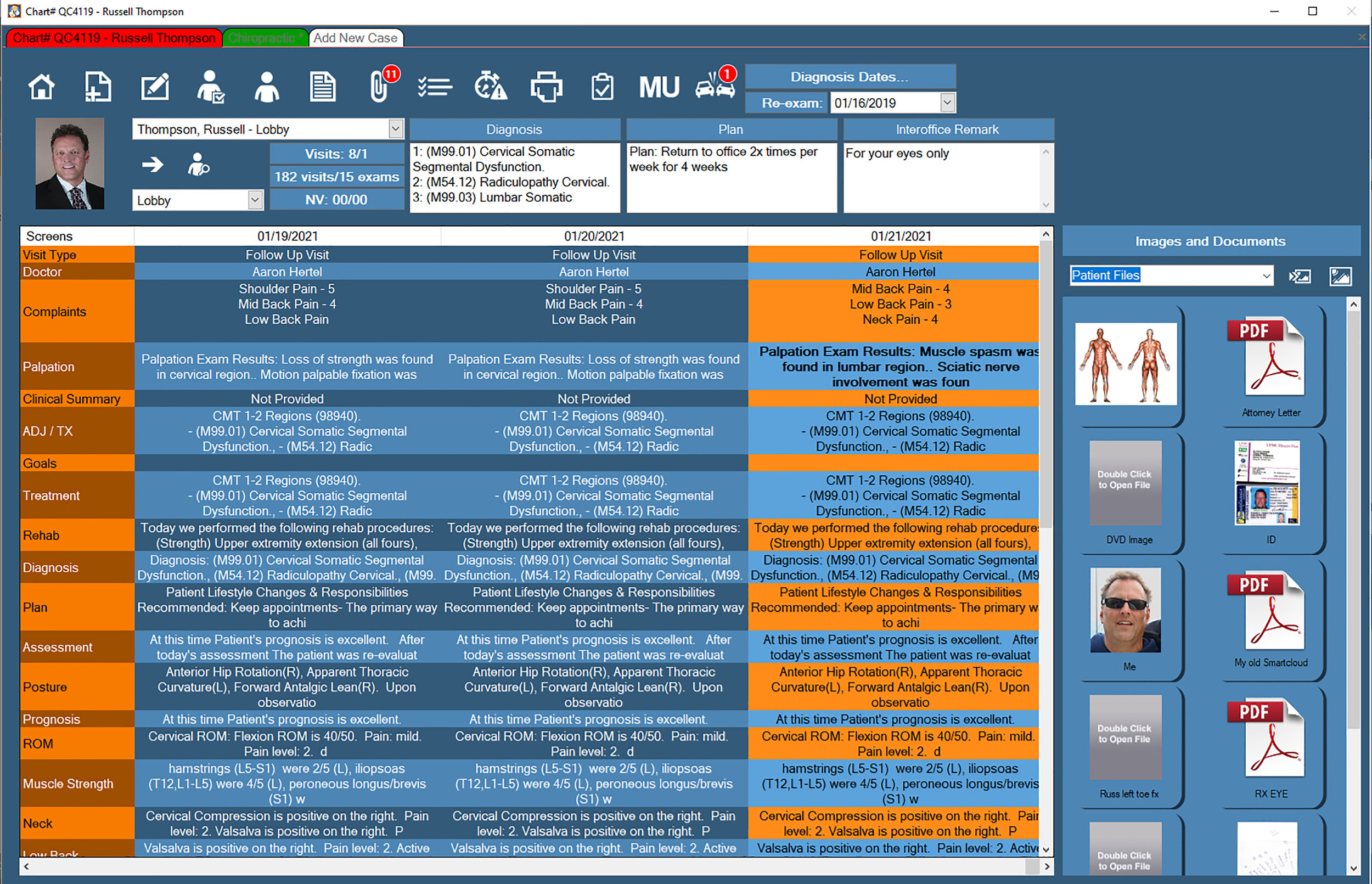
Mastering the SOAP Note Structure
SOAP notes remain the industry standard for chiropractic documentation:
- S – Subjective: Patient-reported symptoms and experiences.
- O – Objective: Measurable findings such as range of motion, posture, or palpation results.
- A – Assessment: Your clinical interpretation or diagnosis.
- P – Plan: The next steps—adjustments, therapies, frequency, and duration.
Pro Tip: Keep Notes Patient-Centric
Avoid copy-paste habits. Each note should reflect that day’s specific findings and progress.
Compliance and Audit-Ready Recordkeeping
Regulations surrounding chiropractic documentation evolve frequently. Stay aligned with your state board’s requirements and payer guidelines to avoid compliance risks.
Common Mistakes to Avoid
- Missing daily notes for active care plans.
- Failing to document patient education or home exercise recommendations.
Omitting time-based procedures.
Streamlining Documentation with Chiropractic Software
A reliable EHR built specifically for chiropractors can drastically improve documentation speed and accuracy. Features like pre-built templates, auto-fill for recurring treatments, and one-click coding ensure consistency across all patient visits.
Benefit Beyond Efficiency
Automation helps you focus more on patients and less on paperwork—increasing satisfaction and retention.
Final Thoughts
Great documentation reflects great care. It communicates your clinical reasoning, supports your revenue, and builds trust with patients and payers alike. By mastering documentation standards and using tools that simplify them, chiropractors can focus on what they do best: helping patients heal.
FAQs
How long should chiropractors keep patient records?
Can I reuse templates for different patients?
How do I prepare for a documentation audit?
Accurate, compliant documentation doesn’t have to be complicated. With structured workflows and reliable systems in place, chiropractors can create records that support both exceptional care and long-term success.
Empower your practice! Get a Free Demo Today!
Experience the power of a personalized demo with our expert software developer. Discover how Quick Charts can revolutionize your chiropractic practice with its seamless integration of cutting-edge technology. From simplified patient management to advanced analytics, our software empowers you to take your practice to new heights. Don’t miss out on the opportunity to see firsthand how Quick Charts can transform your workflow and enhance patient care. Schedule your demo today.